
TRANSARTERIAL BRACHIAL PLEXUS BLOCK
Case Report
Equipment
Drugs
How to proceed ?
Indications
Contraindications
Advantages
Drawbacks
Side effects and complications
Pearls
Costs
The transarterial approach to the brachial plexus (TAB) allows excellent
blockade of the five sensory nerves of the upper limb easily. It is indicated
for procedures on the elbow, forearm, wrist and hand lasting more than
90 minutes, especially if good postoperative analgesia is required.
The transarterial technique described here is the easiest
technique to block the upper limb. It is based on an experience of
1,000 cases per year for more than 20 years. Two different injections
are required : one proximal, transarterial, to block the median,
radial and ulnar nerves ; and a second one a bit more distal, subcutaneous
and intramuscular, to block the medial cutaneous nerve, the intercostal
brachial nerves and the musculocutaneous nerve.
Case Report : :
In contrast to common opinion, TAB is a good option for abcess of the
upper limb (as described for IVRA, see above) at the condition that there
is neither lymphangitis, nor palpable axillary lymph nodes. Even more
so, if a general anaesthesia would be at risk.
Also, all surgeries on elbow, foerarm, wrist and hand lasting
more than 90 minutes. All surgeries on the upper limb, whatever the duration,
if excellent postoperative analgesia is required.
- A 24 G needle.
- A 75 cm extension tube.
- Four syringes : 3 of 20 cc and 1 of 10 cc.
- A sterile set with 2 cups : one for disinfection and one for the solution.
- A standard tourniquet.
- A manometer.
- An Esmarch rubber bandage.
- An IV cannula.
Drugs required for standard TAB (5 hours duration) :
- Epinephrine : 0.4 mg = 2 cc (dilute 1 mg in 5cc Mandatory. Never forget !).
- Carbonated lidocaine 2 % : 50 cc.
- Levo-bupivacaine (Chirocaine) 0.5 % : 20 cc.
- NaCl 0.9 % : 10 cc.
Drugs required for long TAB (12-24 hours duration) :
- Epinephrine : 0.4 mg = 2 cc (dilute 1 mg in 5 cc Mandatory. Never forget !).
- Carbonated lidocaine 2 % : 25 cc.
- Levo-bupivacaine (Chirocaine) 0.5 % : 45 cc.
- NaCl 0,9 % : 10 cc.
- Catapressan : 150 mcg
In both cases, a total volume of 80 cc !
If you have never done it before, try first on simple cases with good landmarks in the presence of an experienced anaesthetist, if possible. Always follow directions carefully !
Preparation :
- Monitor : blood pressure, oxymeter., patient lying flat.
- IV cannula on the contralateral side ; give IV sedation (midazolam 2 mg or Propofol 30-50 mg).
- Inform the patient that two different injections are required. Warn him/her of possible paraesthesia.
Block itself :
- Put arm and forearm on two cushions : arm abducted
to a bit more than 90° and forearm flexed.

- Take landmarks with a marker : the first one on
the axillary artery in the axillary groove (easy to feel), and the second
one higher in the axilla near the pectoralis major muscle. Then, put
sterile gloves on.

- Disinfect the axillary area.
- Position of the anaesthetist : sitting comfortably.
Chest in the axis of the arm ; for a right-handed, put the left
index on the artery high in the axilla and hold the needle between your
right index and thumb, just « like a pen ».

- Remind your assistant that 30 cc will be injected behind the artery and 30 cc in front of the artery. And also that ASPIRATION EVERY 5 CC IS ABSOLUTELY MANDATORY : the tip of the needle can migrate intraarterially during injection !
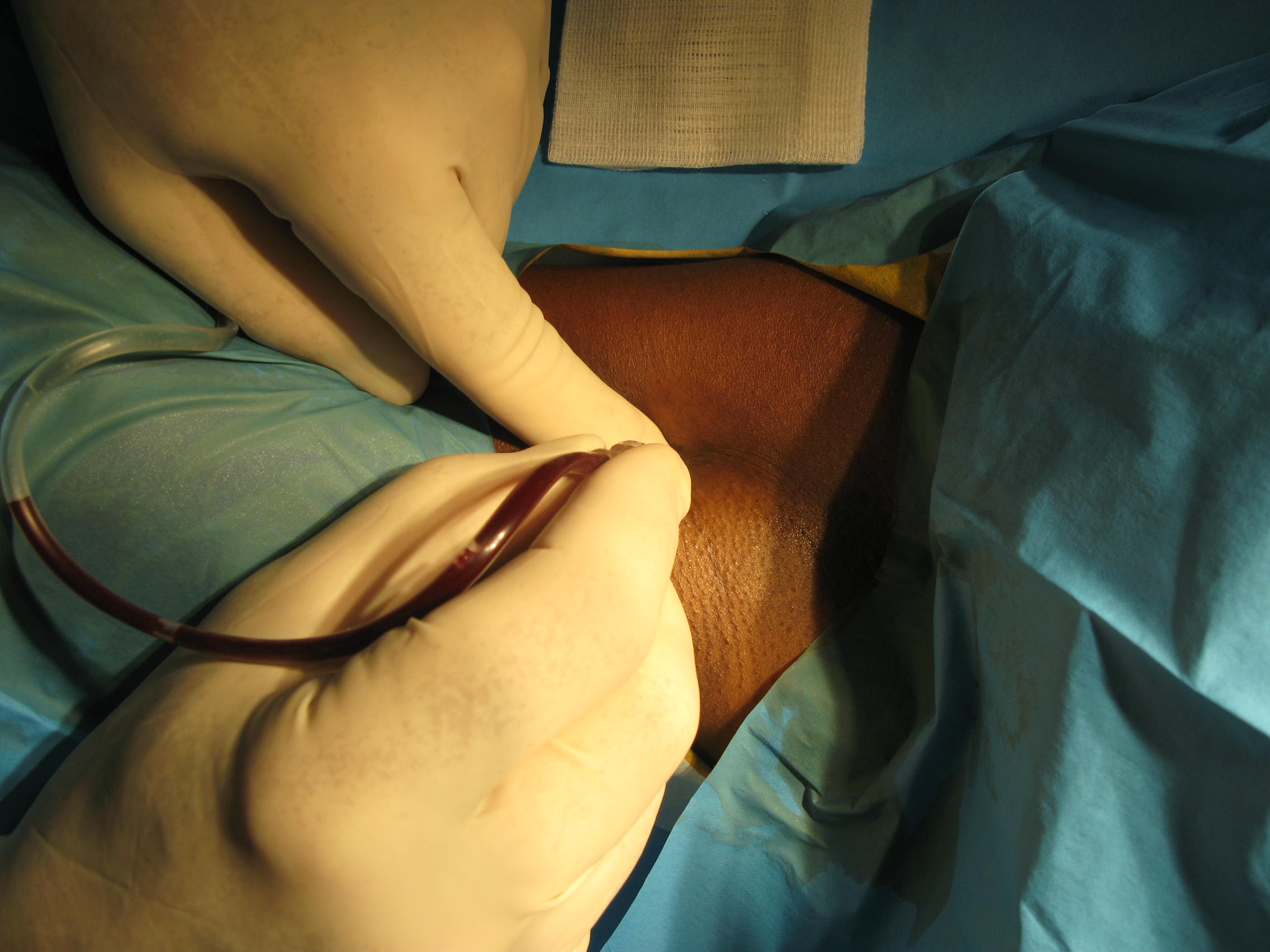
- First injection. Tell the patient that he/she will feel a pinprick and tell your assistant to aspirate. Stick the needle ; once correctly placed, red blood is seen in the tubing.
- Transfixiate the artery until no more blood is aspirated.

- Inject a few cc to clear out the tube.

- Aspirate again to be sure that the tip of the nedle is behind the artery.
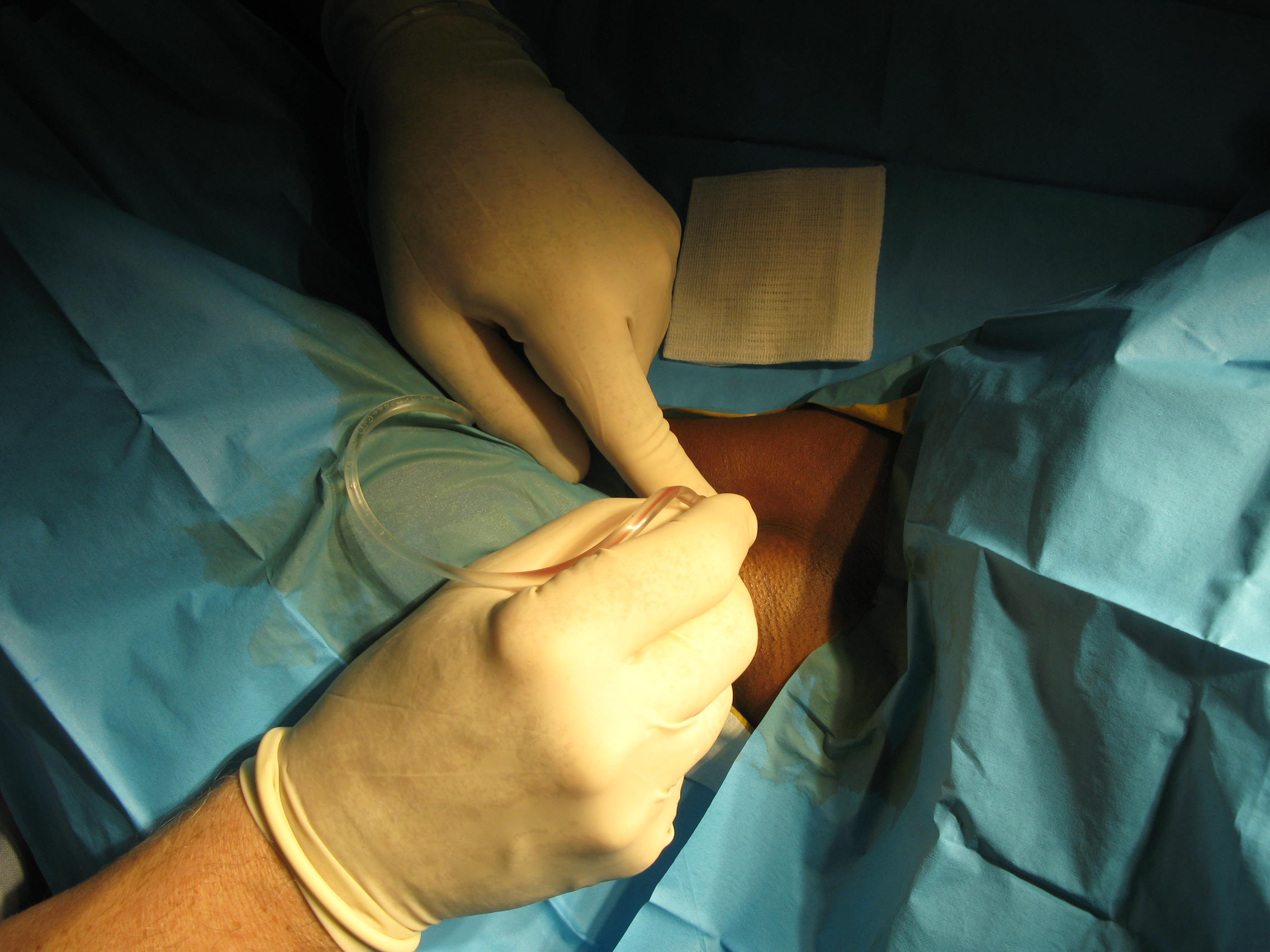
- Ask your assitant to inject 30 cc and to aspirate every 5 cc ; then, to keep aspirating while moving the needle in front of the artery.
- Clear the tubing out again.
- Aspiration.
- If no blood in the tubing, inject 30 cc in front of the artery and aspirate every 5 cc.
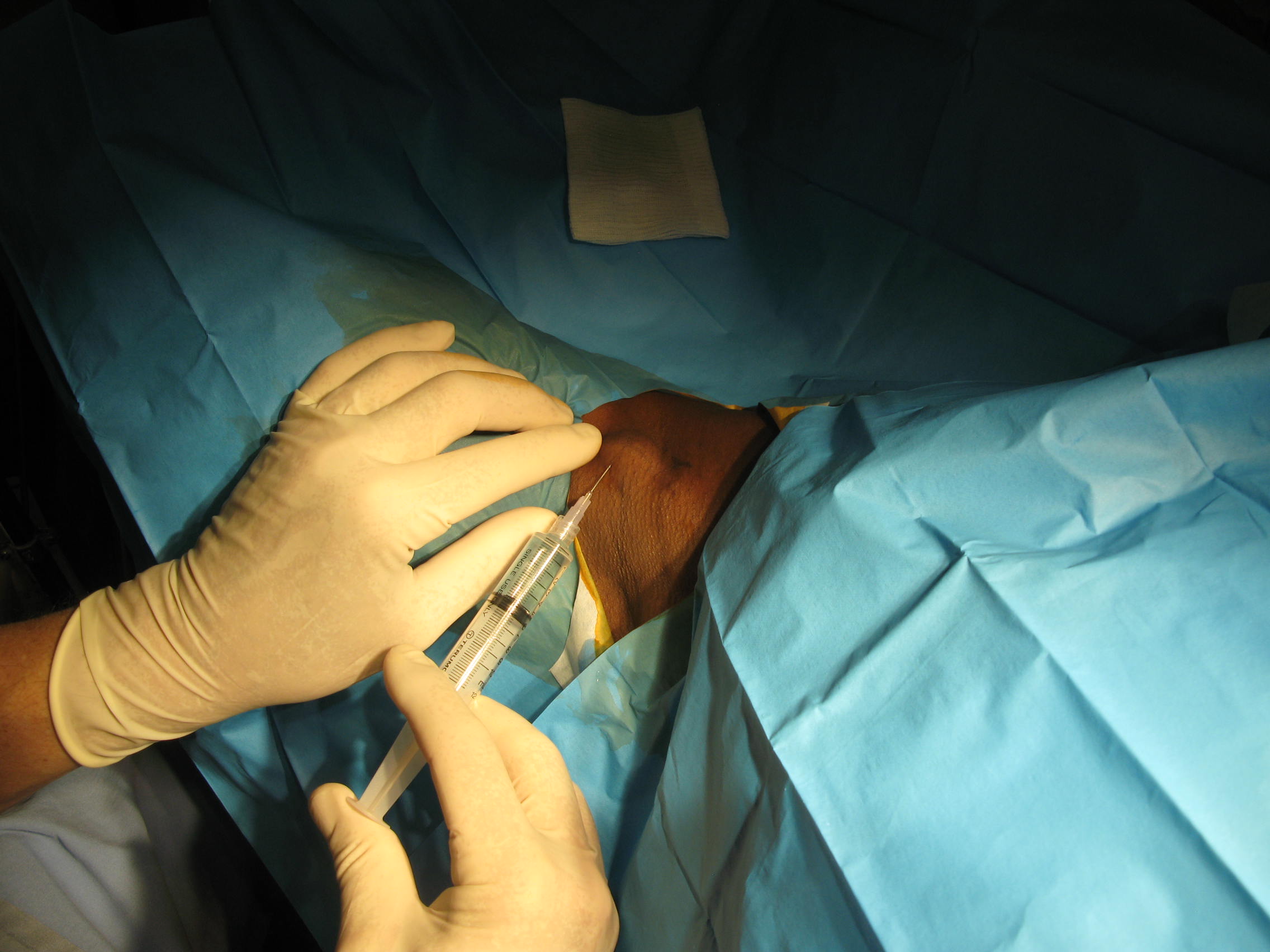
- After injection, disconnect the needle from the tubing and put it on the 10 cc syringe.
- Ask your assistant to hold the patient’s hand. Move yourself by the patient’s chest and warn him/her of the second injection.
- Second injection. Inject about 8 cc subcutaneously :
3 cc on the top of the artery to block the medial cutaneous nerve and
5cc semicircular to block the sensitive branches of the intercostal
nerves.

- Then, stand and pinch the coracobrachial muscle. Stick the needle down to the bone. Then, infiltrate the muscle in a fan-like fashion to block the musculocutaneous nerve (about 8 cc).



After the two injections :
- Apply pressure on the puncture sites. Then, put the upper limb on the chest and warn the patient of the appearance of warmth, tingling and heaviness in the limb within the next 10 minutes.
- Assess the quality of the block by loss of cold sensation within 10 min. on both sides of the forearm, in the hand and on the back of the hand. If cold sensation is lost, surgery can start 20 to 30 min. after the injections.
- Procedures lasting more than 60 min. on elbow, forearm, wrist and hand.
- To provide excellent postoperative analgesia.
- Infection in the axilla.
- Limited abduction of the arm (depends on experience).
- Anticoagulation (PT less than 50).
- No risk of perforating the pleura ; no risk of diffusion into the CSF.
- Can be performed in the presence of antiaggregants agents (aspirin, clopidogrel) if adequate pressure is applied on the puncture sites. No hematoma with this technique in our experience.
- Works by diffusion around the artery ; therefore, no risk of damaging nerves.
- In presence of painful fractures, TAB is much more comfortable for patients than the neurostimulation technique.
- Less easy to learn compared to IVRA but still easy.
- Time to full effect longer than for IVRA but no more
than 20 min. most of the time.
Side effects and complications :
- Shivering within 15 min following the injections due to vascular absorption and CNS stimulation. Rare. Give Propofol 50 mg IV. Convulsions : very rare, can occur if you forget to put epinephrin in your solution !!!
- Infection at the puncture site. Never occured.
- Persistent neuropathies. Theoretical. Paraesthesia may occur during the blok but persistent neuropathies never happened in our very large series. The incidence of neuropathies is not different wether there are paraesthesia during performing the block or not (see references below).
- Tachycardia during or after the injections due to vasculat absorption of epinephrin. Rare. Give Esmolol IV as much as required.
- If touniquet is poorly tolerated, a sterile one can be placed on the forearm.
- If one nerve is not blocked, there are two solutions : infiltrate the nerve again, or do an IVRA with chloroprocaine 40 cc « on the top of the block » (IV cannula, Esmarch band, cuff on). Not « academic » but very effective and often less risky than conversion to general anaesthesia.
- Decrease the doses : in the elderly ; in patients with very thin upper limb.
- If the brachial artery is not palpable (rare), give ephedrin 10 mg IV.
- If, during performing the block, venous blood is seen in the tubing, do not inject ! A transvenous block is inadequate most of the time..
- Tourniquets : same as for IVRA, see above.
- Lidocaine CO2 2 % SINTETICA : 1 vial x 20 ml : 4.80 Swiss francs (about 5 US dollars).
- Chirocaine (levo-bupivacaine) 0.5 % ABBOTT : 1 vial x 10 ml : 6.44 Swiss francs (about 7 US dollars).
- Extension tube. Type : HEIDELBERGER, Extension line, sterile, Luer Lock, 75 cm : 0.50 Swiss franc a piece. B/Braun. www.bbraun.com.
- Needle 24 G. B/Braun. Sterican. Hypodermic needle.
References :
Hudson et al. : The transarteriel brachial plexus block for hand and forearm surgery : a review of 1062 cases. Eur J Anaesth 2006 ; 24 : 470-471.
Selander et al. : Paresthesiae or no paresthesiae ? Nerve lesions after axillary blocks. Acta Anaesthesiol Scand 1979 ; 23 (I) : 27-33.
Sites et al. : Incidence of local anesthetic
systemic toxicity and postoperative neurologic symptoms associated with
12,668 ultrasound-guided nerve blocks : an analysis from a prospective
clinical registry. Reg Anesth Pain Med. 2012, 37 (5) : 478-482.
