
INTRAVENOUS ANALGESIA with CHLOROPROCAINE
Case Report
Four variations of IVRA
Equipment
Drugs
The syringes
The doses
How to proceed ?
Indications
Contraindications to IVRA
Advantages
Drawbacks
Complications
Pearls
Costs
The administration of intravenous chloroprocaine in an isolated limb by
means of an ischaemic cuff is called intravenous regional anaesthesia
(IVRA). IVRA is ideally suited to operations of the hand, forearm, elbow,
and foot.
Case Report :
A 60 year-old, 130 kg (280 lb) man arrives at 11 PM in the emergency room
with a big abcess of the hand. He is not fasting, smokes one pack a day,
has other comorbidities (Hypertension, Obesity, Sleep Apnea,…). The
surgeon wants to incise and drain the abcess ; he has a long list
the next morning. The operating theater is available and the team is ready.
The anaesthetist is on his own. The recovery room is closed until the
next morning.
Which technique is best ? In contrast to common opinion, I decided
to do an IVRA with two cuffs on the arm which allows to put a third sterile
cuff on the forearm during the procedure if the operation is longer than
anticipated. After inflation of the proximal cuff, I injected intravenously:
chloroprocaine 0.5 % 120 cc + Ketorolac 30 mg + Bicarbonate (see "The
doses" below). After 20 minutes, I inflated the distal cuff on the
arm (and deflated the proximal one). A third cuff on the forearm was not
necessary. At midnight, surgery was all over. The patientt left the hospital
30 minutes later and was asked to come back the next dax for dressing
change.
In contrast to common opinion, a regional technique for infections of
the upper limb, such as IVRA, is a very good choice. A TAB would have
been another option (see below).
Four variations of IVRA with
the same equipment :
- The mini-technique : one single cuff on the forearm.
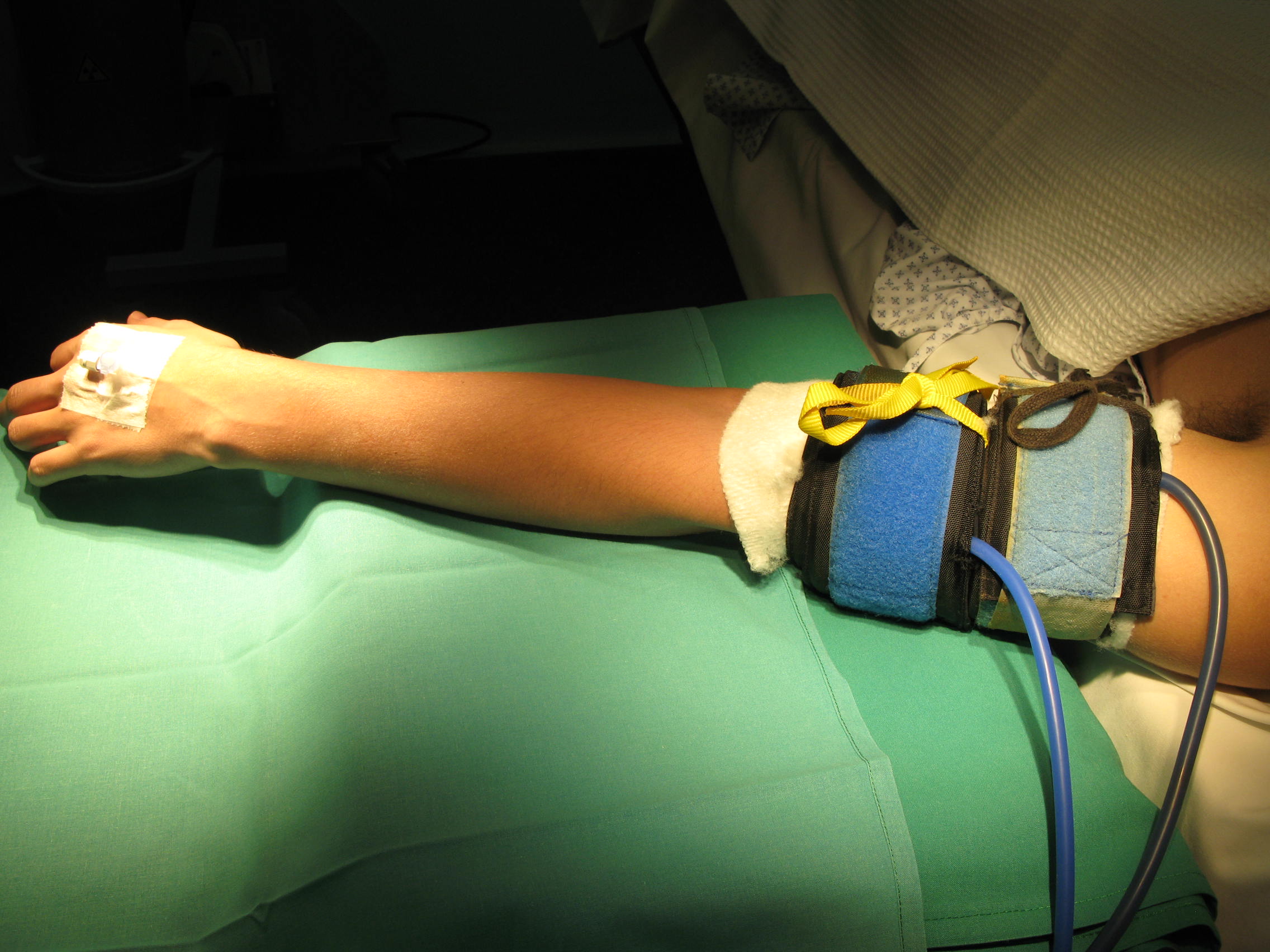
- The two separated cuffs technique : one on the arm, the other on the forearm.
- The two cuffs technique, both of them on the arm.
- The foot technique, both cuffs on the ankle or calf.

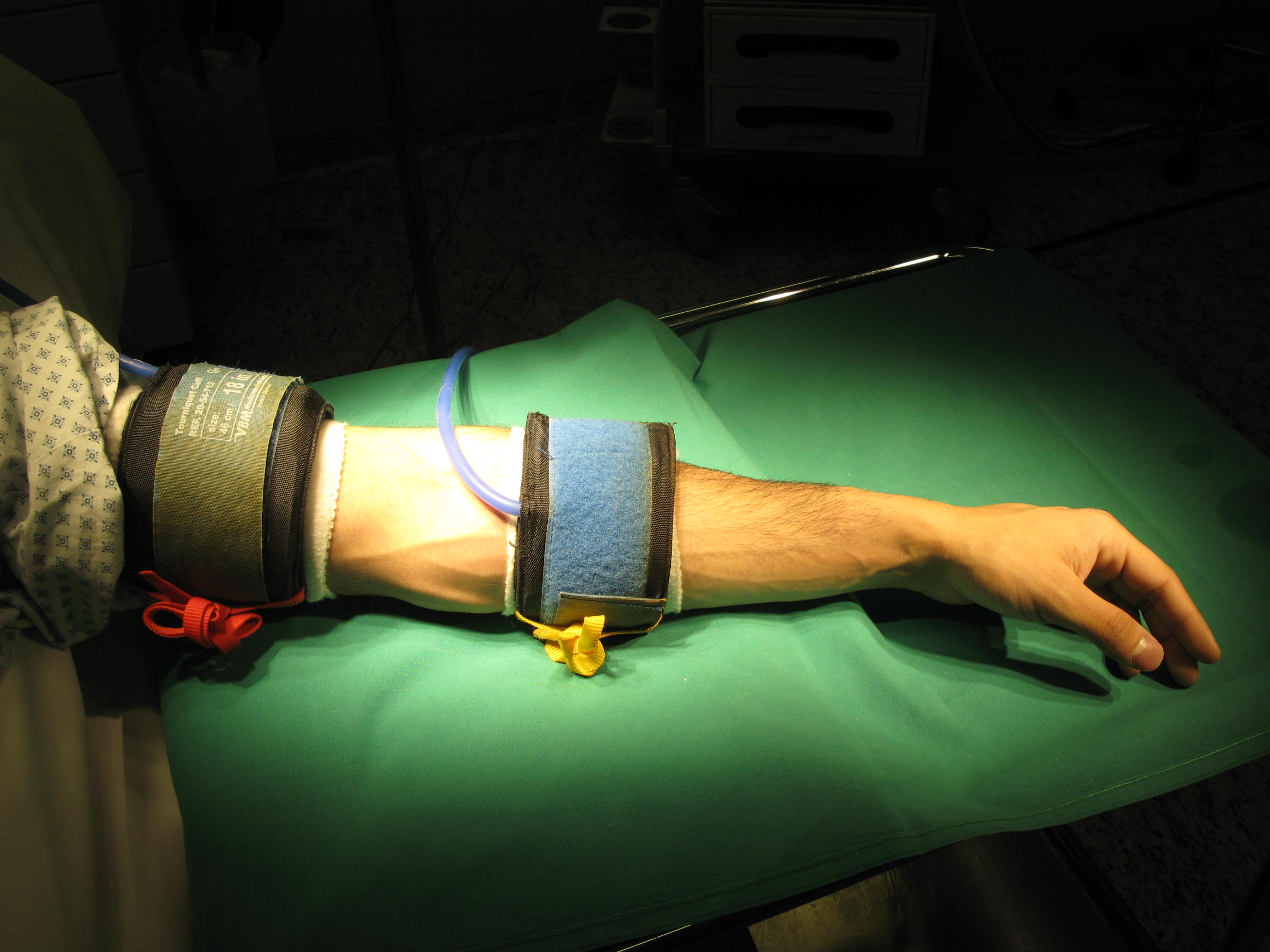

Equipment (for suppliers, see below) :
- Cuffs must be of very good quality
. One of average size for the arm (red laces : 18 in. ; 46
cm) and a smaller one for the forearm or the arm (yellow laces :
14 in. ; 35 cm).

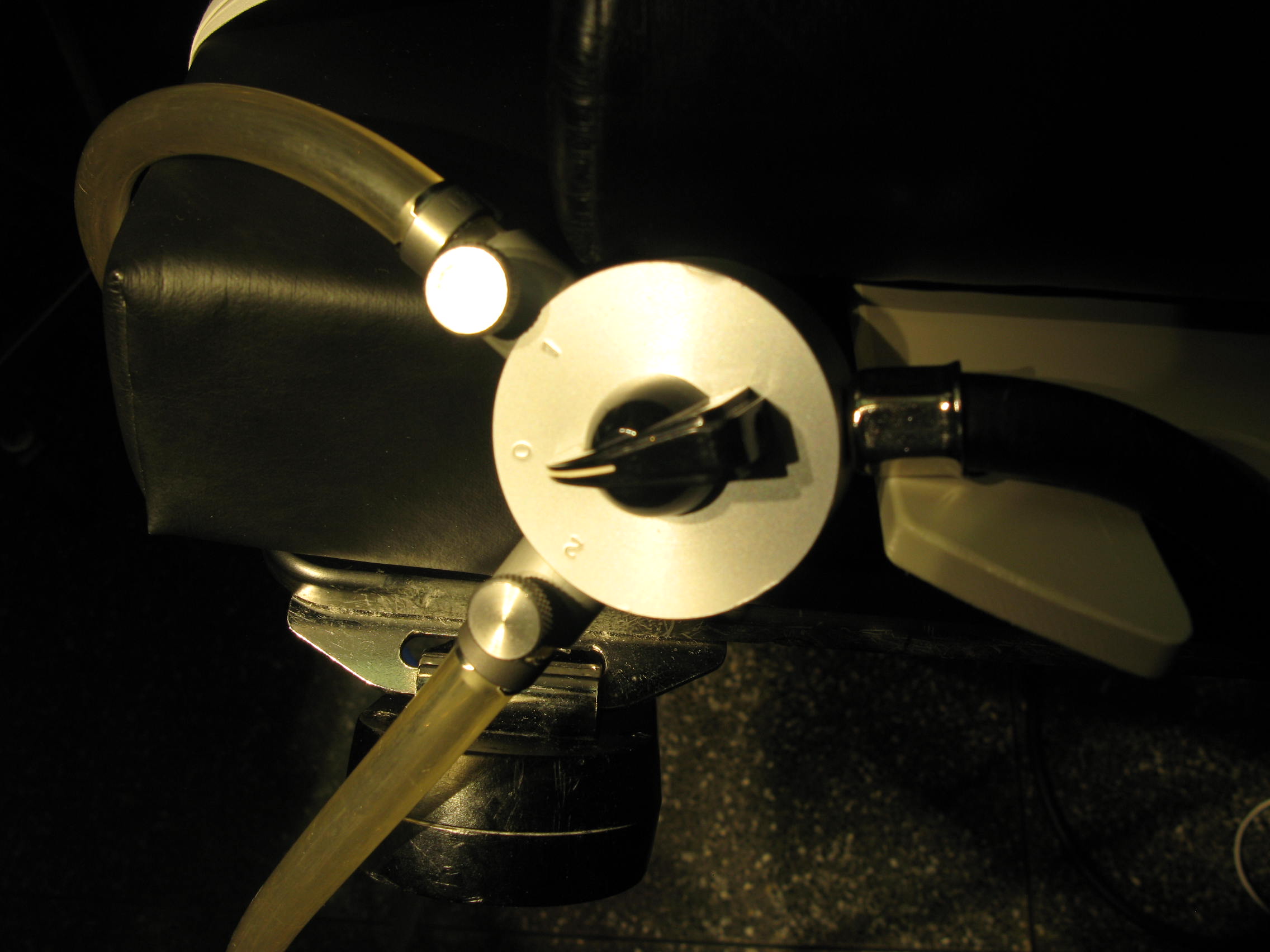
- A reliable two-way stopcock, like the metallic Braem
one.

- A standard manometer.
- An Esmarch rubber bandage.
- Two intravenous cannulae : one for venous cannulation
distal to the cuff (22 G on the hand ; 24 G on the foot) and one
for cannulation in the opposite arm in the event of complications (optional
for the mini-technique).

- Chloroprocaine 0.5 % is the only local anaesthetic agent I use.
- Bicarbonate 8.4 % to prevent the discomfort at the beginning of the injection and to facilitate the local anesthetic effect.
- Toradol (Ketorolac) for postoperative analgesia.
The syringes are injected in the following order :
- One 25 cc syringe: chloroprocaine 0.5 % 20 cc + Bicarbonate 8.4 % 5 cc.
- One 21 cc syringe : chloroprocaine 0.5 % 20 cc + Toradol 1 cc (30 mg).
- The next ones of 20 cc : pure
chloroprocaine 0.5 %.
The doses of chloroprocaine 0.5 % are the following :
- Mini-technique (one cuff on forearm): 0.5 cc to 1 cc/kg (2.5 to 5 mg/kg).
- The two-cuffs technique: 1 to 1.3 cc/kg (5 to 6.5 mg/kg).
- The highest doses are recommended for infections !
- For surgery on the foot, up to 80 cc in adults.
Preparation :
- Monitor : Blood Pressure measurement and Oxygen saturation.
- Check the manometer : pressure must be 100 mmmHg
above the
patient’s systolic blood pressure. - Bilateral venous cannulation.
- Inform the patient. Give IV sedation if required.
IVRA itself :
- First tourniquet : on the forearm for the mini-technique at a 3-digit distance from the elbow ; on the arm for the two cuffs technique.
- Exsanguinate the limb with an Esmarch rubber band, all
the way down to the tourniquet. If it is too painful (fractures…),
simply elevate the
limb for a few minutes with compression of the brachial artery.

- Inflate the cuff to 100 mmHg above the systolic blood
pressure
(250 mmHg) - Injection of the anaesthetic with the patient’s arm in a comfortable position. Inform the patient that the limb will feel a little strange : temperature change, tingling in the fingers, mottled in appearance. Then, remove the IV cannula and apply pressure on the puncture site.
- Lower cuff : put it either just besides the uppermost
one for surgery on the elbow/forearm ; or on the forearm for surgery
on the wrist/hand.

Surgical procedure :
- Disinfection and draping.
- During the procedure. When two tourniquets are used,
inflate the
lower one after 30 to 45 minutes depending on patient’s tolerance
and then deflate the uppermost one. - Inform the patient that the hand will feel a little strange..
- At the end of the procedure. Deflate the lower tourniquet.
For very
short procedures using the mini-technique, the minimum theoretical
inflation time is 20 minutes for the amides, like lidocaine. However,
for esters, like chloroprocaine, the cuff can be deflated after 10 min.
Check blood pressure, pulse and oxymetry one more time. Tell the
patient he is going to feel tingling in the fingers for 15-20 minutes.
- Mini-IVRA : all procedures on hand or wrist of less than 45 minutes.
- Double cuff on the calf : for foot procedures of less than 60 minutes.
- Double cuff on the upper limb : all procedures of less than 90 minutes.
- In contrast to common opinion, IVRA is very effective for infections at the condition that high doses are used.
- Pediatrics : IVRA well tolerated at the age of
6 or older. Put anaesthesia cream (EMLA) on both hands for IV cannulae.
Explain carefully.
- Absolute : Allergy to Toradol. Just use chloroprocaine and bicarbonate.
- Relative : Allergy to local anaesthetics :
none with IV chloroprocaine (very rarely, weals disappearing quickly).
Psychological : to be discussed with the patient.
- Theoretical : plasma esterase deficiency. In our practice, the limb always gets back to normal in a few minutes.
- The anaesthetist can work on his/her own, with no extra-hands, with no induction room.
- Patients should not be starved.
- Can be used in the presence of aspirin or clopidogrel.
- Simplicity (can be learned very quicly ; follow directions carefully !).
- Save time.
- Very effective method.
- Patient’s satisfaction.
- Recovery time. In all cases, limb back to normal in minutes due to chloroprocaine very short half-life. Most patients leave the hospital 30 min. after the procedure.
- Low cost (see below).
- Works by diffusion ; therefore, no tissular lesion, except a small hematoma at the site of the cannula.
- Tourniquet pain. Time limitations : 45 min. for the single cuff ; 60 min. for the foot ; 90 min. for the double cuff on the upper limb. Give propofol IV if necessary.
- Cuff tolerance is variable. Even children are amenable to IVRA alone. To be combined with sedation and additional analgesia if necessary.
- At cuff deflation, tingling in the fingers for 15-20 minutes. No residual analgesia.
- Registration : chloroprocaine not registered for IV use in some countries.
- Dizziness during injection (rare): very short-lasting (1 to 2 min.) with a mild increase in heart rate (due to chloroprocaine bypassing the tourniquet). Just reassure the patient ! At deflation, very rare.
- Vagal reaction due to stress and/or tourniquet pain.. Give Atropine 0.5 mg IV ; have a second dose ready. Reassure the patient. Rare.
- Theoretical : shivering/convulsions. Never observed.
- IV cannulation for IVRA can be inserted at the level of the elbow if no vein can be found more distally. The injectate flows backwards.
- Cuffs must be of very good quality. Ensure that they do not leak. Monitor cuff pressure.
- Sterile cuff can be placed on the forearm, as a third cuff, if procedure longer than expected (double cuff on arm technique).
- Surgeon must be aware that a small dose of lidocaine subcutaneously may be necessary at incision (rare).
- Obesity : give an intermediate dose first, then test the analgesia. Give more if inadequate.
- Non-sterile cuffs : VBM simple manchette with silicone balloon. Intermediate size (14 in.) : about 130 US dollars ; big size (18 in.) : about 160 US dollars. Sold by Laubscher (www.laubscher.ch). E-Mail : info@laubscher.ch.
- Sterile cuffs : VBM Brassard simple Dispo Cuff, sterile, 18 in. : about 20 US dollars (www.laubscher.ch). E-Mail : info@laubscher.ch
- Two-way metallic stopcock : about 230 US dollars. Sold by H.P. Braem AG, article n° 100600. Direct contact by phone : - 41-71 866 1933 (ga@hpbraem.ch)
- Chloroprocaine 0.5 % (Ivracain) 5 amp x 20 ml : about 30 US dollars. Sold by Sintetica S.A (www.sintetica.com). E-Mail : info@sintetica.com.
Reference :
Van Zundert A. et al . Centennial of Intravenous
Regional Anesthesia. Bier’s Block (1908-2008). Reg Anesth Pain
Med 2008 ; 33 : 483-489.
